A pediatrician and a mother share sobering lessons learned regarding water safety for children.
Hughes: My 3-year-old son, Levi, drowned in June 2018 while we were on a beach vacation with friends. One moment, he was sitting on the couch watching TV. In the next, I was pulling his lifeless body from the bottom of a pool.
Levi had somehow slipped out of a living room filled with children and adults, including myself, my husband, and 5 physician friends. We weren’t drinking, weren’t on our phones, and had finished swimming for the day.
I was the one who glanced over the balcony and found our Levi, my guttural screams bringing a rush of people outside. My husband, a cardiothoracic anesthesiologist, was the first to perform cardiopulmonary resuscitation (CPR) on his only son.
The confusion of “but we weren’t even swimming” and “Levi was just on the couch” hung in the air as we grappled to make sense of the senseless. It happened so quickly. However, despite immediate attention, including advanced resuscitation from multiple physician experts, we lost our Levi.
Porter: At the age of 3, Levi Richard Hughes joined over 400 other children across the United States between ages 1 and 4 years who die annually from unintentional drowning.1 Although it only takes 20 seconds for a child to drown,2 it has been an unconscionable 3 decades of stagnant drowning rates for this vulnerable population.
Levi’s death was not unlike other drownings of children his age. Given his developmental stage of life, he chose to explore his surroundings and met his ultimate fate in the pool, where the majority of drowning fatalities of children ages 1 to 4 years occur1 during moments when the child was not expected to be swimming.3
Hughes: How did our son drown? How were years of intentional parenting seemingly nullified within seconds?
Levi’s death rests on my husband and myself. There is no denying that we failed to keep him safe. But I have since learned that water safety goes far beyond the assumed foolproof advice of simply “watch your kids while swimming.”
Parents only know what they know. I thought I was doing everything right to keep Levi safe. I have 16 photos of what would be my son’s final day of life; in 14 of them, he is wearing a life jacket. These are time-stamped photos of my precious boy, grinning proudly, secured in his personal flotation device.
I will never stop wishing I had not momentarily turned to clean up dinner or that I had seen Levi slip out the door that night. However, I have come to believe I made another grave mistake that significantly contributed to my son’s death: I encouraged Levi to believe that water was fun. We don’t stand in streets or busy parking lots and eagerly proclaim to our impressionable toddlers, “Come on in—the traffic is fine.” We don’t encourage our kids to play with real guns in an effort to make them “comfortable” around firearms. Yet this is exactly what we do with water, a substance just as deadly as streets, parking lots, and guns.
Porter: For many children, the concept of “water is fun” is introduced in infancy, encouraged by playful splashing in bathtubs. Parents may take their toddlers and preschool-aged children to swimming pools and cheer on their child’s developing comfort in and around the water. Children may even be enrolled in formal swim lessons recommended by family, friends, or a medical provider. These early water engagements have a similar purpose—that children become comfortable in water4,5—and yet parents are unknowingly increasing their child’s comfort and joy around a substance that kills thousands of children each year without also providing the skills to survive.6 Conventional wisdom has promoted early and gradually increased positive water exposures, followed by swim lessons when a child is ready. “When a child is ready” and the type of swim program are of critical importance and yet unclear.
Currently, the American Academy of Pediatrics (AAP) advises families follow the advice of their child’s pediatrician to determine the appropriate age for formal lessons. Parents may be advised to consider swim lessons after the child’s first birthday, taking into consideration the child’s emotional, physical, and developmental abilities and comfort in the water.7 However, experts only begin to agree that most children are ready for swim lessons by their fourth birthday, which is long after the highest risk age of drowning.7,8
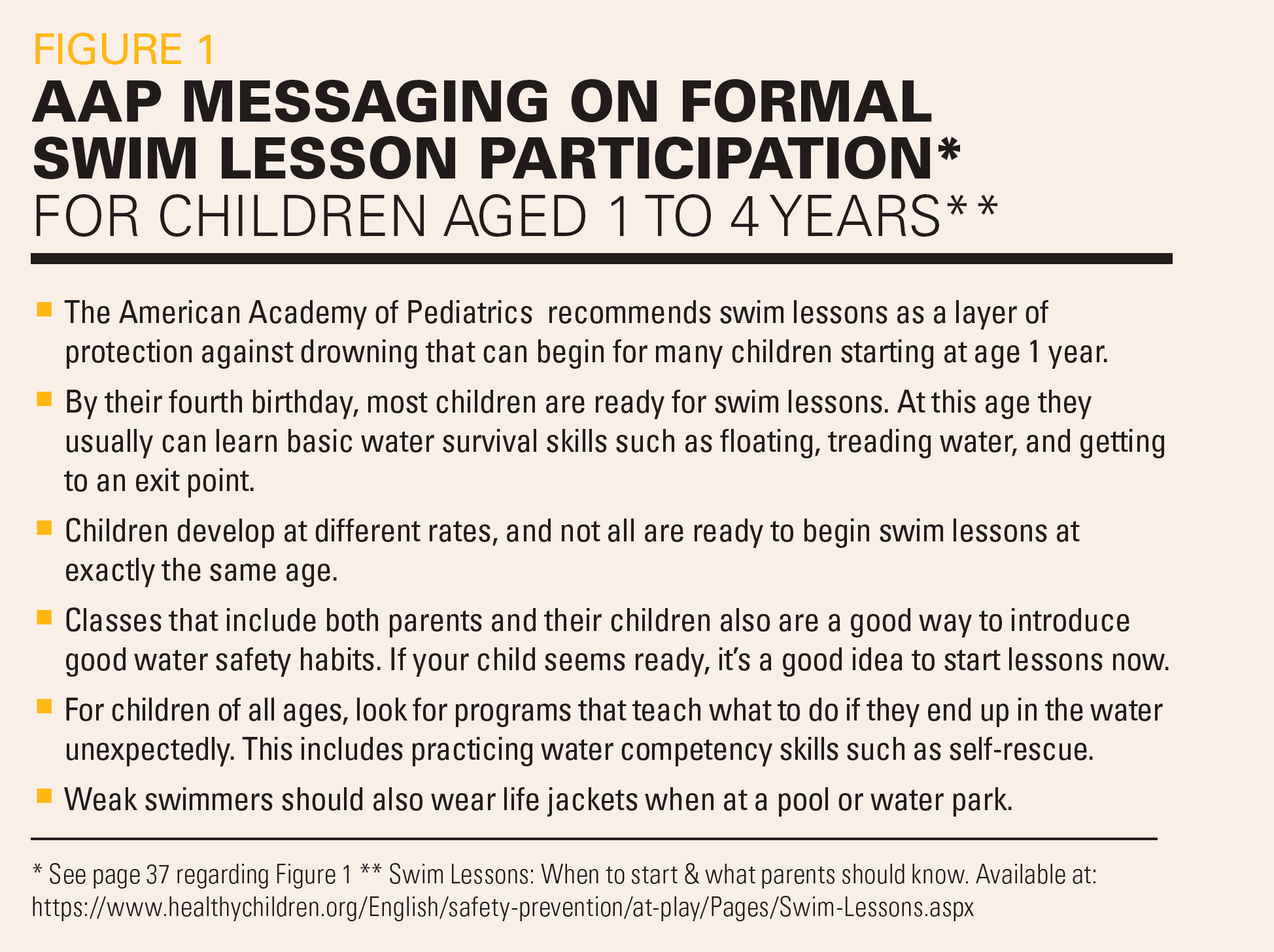
Significant variability in the type of swim programs also exists,9 with experts conveying that not every program will be right for each child.8 Parent-led classes are endorsed for children aged 1 to 4 years to build swim-readiness skills. Simultaneously, parents are advised to consider programs that teach self-rescue skills and encouraged to use life jackets in the pool if the child is considered a weak swimmer.7
Figure 1 highlights AAP’s swim lesson messaging according to a child’s age and types of swim programs that, for many parents and pediatricians, can appear confusing and conflicting. This lack of consensus may contribute to the infrequent drowning prevention conversations that are given by pediatricians during well-child visits.10,11 We agree with the AAP that a broad and coordinated research agenda is needed to address the efficacy of type of swim lesson programs for children aged 1 to 4 years.8
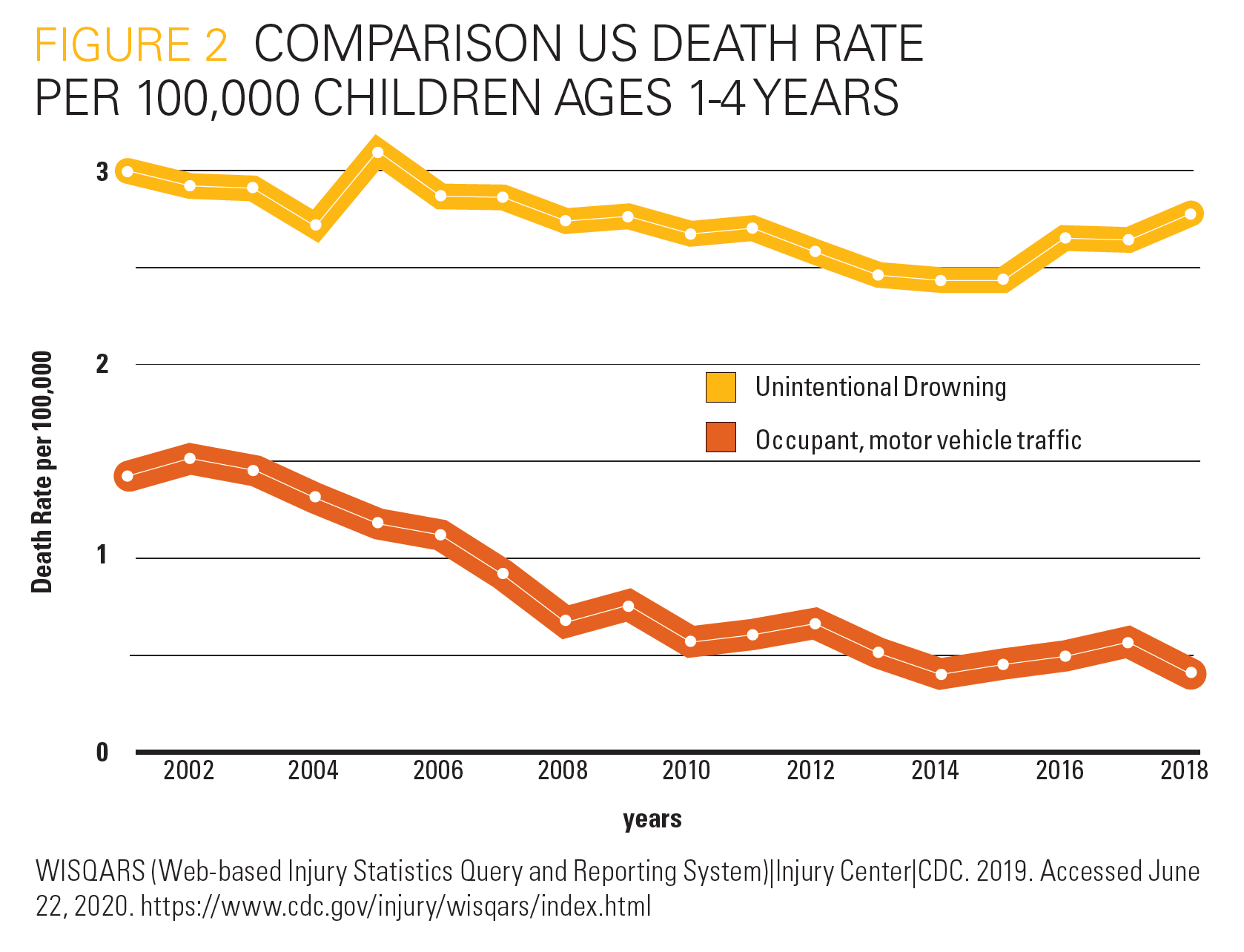
Hughes: The stigma around drowning is the greatest threat to prevention efforts. Clearly our culture’s current approach to drowning prevention is not working. Although advancements in child safety have been seen in other areas, drowning safety has watched from the sidelines (Figure 2). The same water safety tips are casually tossed out each year: Watch your kids while swimming. Install a fence. Buy a life jacket. Wait until children are “ready” to start swim lessons. Learn CPR.
Levi was not swimming. He was wearing khaki shorts and sitting on a couch a moment before he drowned. The beach house had an isolation fence with a self-latching gate. Levi always wore a life jacket when in the pool. We had researched and followed AAP recommendations to wait until the age of 4 years for formal swim lessons. He had 6 physicians by his side within seconds of being pulled from the water. Yet none of these things saved him.
Porter: It is well accepted that drowning prevention involves layers of protection (restricting access to water, supervision, learning to swim, use of lifejackets, CPR) and that enacting all layers achieves the best protection.12 It is also noted that at least 1 layer of protection is breached in 9 out of 10 fatal pool drowning cases.13 One layer of protection that is not often discussed but clearly contributed to Levi’s death was his lack of water competency.
Operationalized concepts of water competency14,15 have historically included elements such as the ability to float and tread water. However, these 2 elements are not of equal importance because floating requires less energy expenditure than treading water16,17 and lack of floating ability has been voiced by drowning survivors as a threat to life and reason for rescue.18 Lack of these competencies may help explain the unchanging drowning rates for children ages 1 to 4 years but are rarely a part of drowning prevention conversation for this population.
Hughes: We must remember that children, not parents, are the true victims of drowning. We owe it to our children to know better and to do better.
We start by looking at success stories in prevention of other premature childhood deaths. For example, as pediatric deaths from motor vehicle crashes rose, we didn’t keep the same approach year after year and hope for the best; instead, we looked beyond the norm and pushed for radical change with the manufacturing and regulation of car seats. Now car seats save thousands of children from preventable injury and death every year.
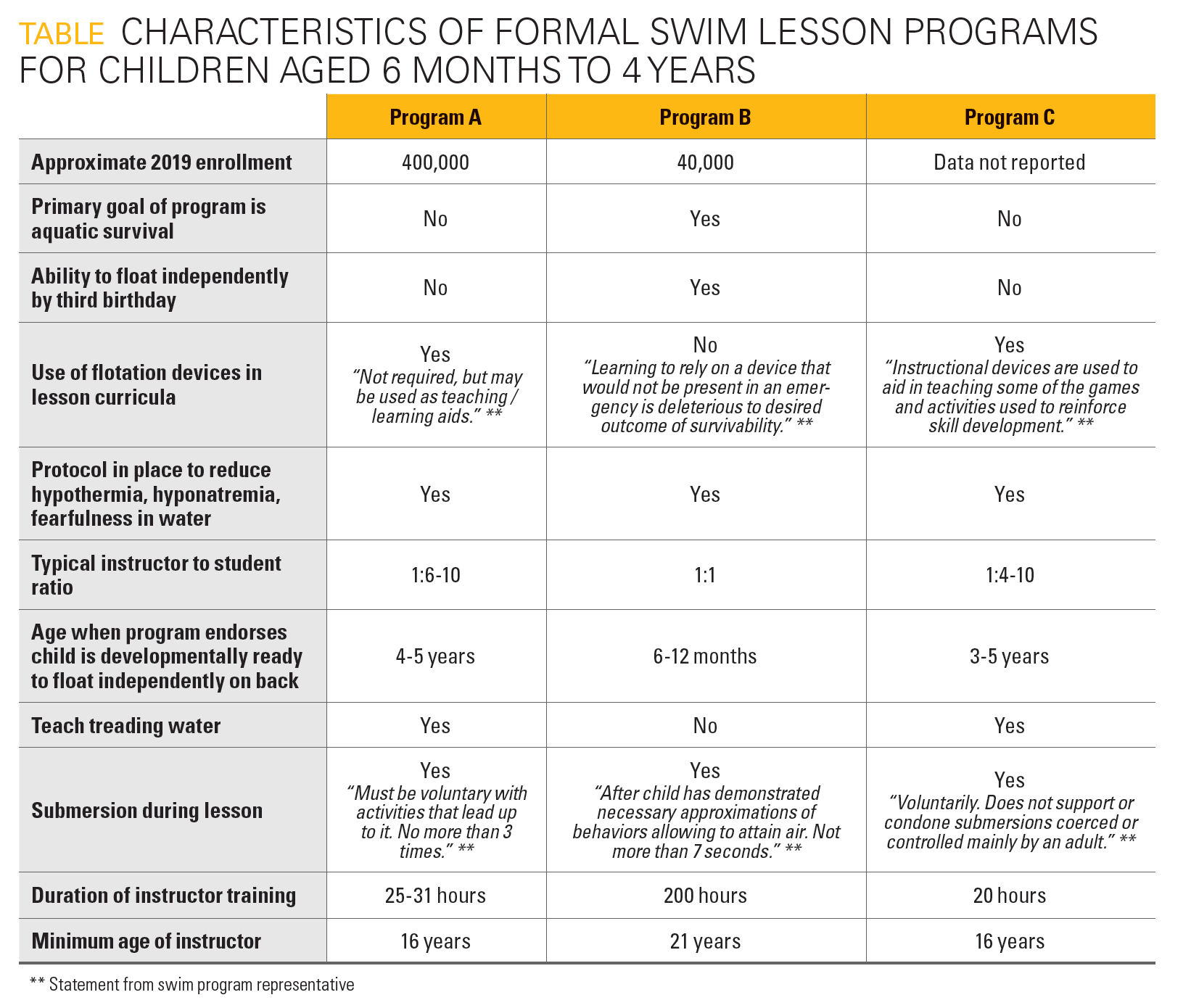
Porter: To better understand our nation’s current drowning approach as it relates to water competency, we reviewed curricula of 3 popular US swim lesson programs. Programs A and C represent parent-led group lessons typically taught in city recreation centers whereas Program B is a survival swim lesson model taught in public or private pools. Our main objective was to compare these programs’ goals and methodologies for achieved water competency of children aged 6 months to 4 years. The Table summarizes key data elements shared by these programs; results are intended to help caregivers and providers determine which program best meets their child’s water exposure needs.
Review of these programs reveal significant differences in water competency intent and instruction. Although tens of thousands of toddler and preschool-aged children participate in programs A and C, neither of these programs has a goal of water survival at this age. Program B focuses on water survival with significantly more hours dedicated to instructor training and certification as well as a 1:1 instructor-to-child ratio during class. Program B’s methodology also avoids use of flotation aids and teaching of treading water, both of which orient the child in a vertical position thereby inhibiting children’s reliance on their own natural buoyancy.
Hughes: After Levi drowned, I heard about swim programs that taught babies how to float. Hundreds of parents reached out to me to share their passionate testimonials of how these swim lessons saved their children. I was admittedly skeptical. However, as I continued to research pediatric drowning, I saw consistent factors: Children who drown usually loved water, they had relied on a flotation device when swimming in pools, and they did not know how to survive if they reached water alone.
My perception of water shifted, and on the exact day that marked 20 months since Levi’s death, we handed over our 8-month-old daughter Willow, Levi’s little sister, to her first Infant Swimming Resource lesson. I watched her take on water and win. She was not just trained to float; she learned to roll her infant body, find the surface, and get air. Even beyond her ability to survive in water, Willow began to develop a lifetime respect for water.
Porter: Although survival swim has existed for decades, it has been less well adopted and accepted within the water safety community. This perspective may be due in part to 1 historical case report of prolonged exposure to water resulting in infant hyponatremia;19 but may also be further perpetuated by the notion that survival swim causes children emotional trauma.
Interestingly, what stands out in our review is survival swim’s rigorous instructor training and private lesson approach. Instructors are trained in methodologies based in behavioral science, sensorimotor learning, schedules of reinforcement, and the building of behavioral chains with the goal of teaching infants and toddlers to learn skills to help them float and find air if met with an unplanned submersion. Although further research is needed to provide evidence on drowning prevention effectiveness comparing differing swim lesson programs, survival swim (program B) currently is the only methodology that aims to teach aquatic survival skills to children aged 12 to 36 months, which are at highest risk age for drowning.
The statistics prove that our national approach to drowning prevention is failing. We cannot continue to only emphasize and rely on environmental barriers to prevent drowning among young children; rather, we must include the critical piece of water competency for children aged 1 to 4 years in the event of an unintended submersion. As stated by Stallman et al, “The causes of drowning should dictate the way we teach swimming, what children should learn.” Yet “an unfortunate number of teachers or schools emphasize that which is popular with parents” and perhaps not what actually saves lives.18
It is time to reframe our drowning prevention approach from focusing on enjoyment during early water exposures to prioritizing the sole layer of protection that always accompanies the child—their water competency. We must reconsider how and when we teach infants and young children arguably the most vital aquatic skill they can learn: independent back floating. We must reassess swim programs’ success based on demonstrative acquisition of this aquatic survival skill so that pediatricians can provide parents more clear messaging on the timing and type of formal swim lesson enrollment, especially in this most high-risk age. Pediatricians also need to discuss with parents, starting with when their children are infants, that how children are introduced to water and taught to interact with it are just as important as the skills they are taught in it. Encouraging the young child to jump into your arms in a pool with a flotation device can teach them that it is safe and fun to enter and submerge in water that, absent adult supervision has the ability to quickly kill them.
Hughes: Drowning statistics have remained relatively unchanged over decades. Now, we have the power to fix this drowning epidemic. It is time to provide toddlers, our children most at risk of drowning, with the ability to roll, to float, and to survive.
References
- WISQARS (Web-based Injury Statistics Query and Reporting System)|. Centers for Disease Control and Prevention. Updated July 1, 2020. Accessed May 2, 2021. https://www.cdc.gov/injury/wisqars/index.html
- National Water Safety Program. US Army Corps of Engineers. Accessed May 2, 2021. https://www.usace.army.mil/Missions/Civil-Works/Recreation/Water-Safety/videoid/548968/
- How to plan for the unexpected: preventing child drownings. US Consumer Product Safety Commission. Accessed May 2, 2021.https://www.cpsc.gov/s3fs-public/359.pdf
- Moran K, Stanley T. Parental perceptions of toddler water safety, swimming ability and swimming lessons. Int J Inj Contr Saf Promot. 2006;13(3):139-143. doi:10.1080/17457300500373572
- Moran K, Stanley T. Toddler drowning prevention: teaching parents about water safety in conjunction with their child’s in-water lessons. Int J Inj Contr Saf Promot. 2006;13(4):254-256. doi:10.1080/17457300600678201
- Global report on drowning: preventing a leading killer. World Health Organization. 2014. https://apps.who.int/iris/handle/10665/143893
- Swim lessons: when to start & what parents should know. healthychildren.org. Updated March 15, 2019. Accessed May 2, 2021.https://www.healthychildren.org/English/safety-prevention/at-play/Pages/Swim-Lessons.aspx
- Denny SA, Quan L, Gilchrist J, et al; Council on Injury, Violence, and Poison Prevention. Prevention of drowning. Pediatrics. 2019;143(5):e20190850. doi:10.1542/peds.2019-0850
- Carr WD. Formal swimming lessons must be defined. Arch Pediatr Adolesc Med. 2009;163(10):961-962; author reply 962. doi:10.1001/archpediatrics.2009.184
- O’Flaherty JE, Pirie PL. Prevention of pediatric drowning and near-drowning: a survey of members of the American Academy of Pediatrics. Pediatrics. 1997;99(2):169-174. doi:10.1542/peds.99.2.169
- Olson LM, Inkelas M, Halfon N, Schuster MA, O’Connor KG, Mistry R. Overview of the content of health supervision for young children: reports from parents and pediatricians. Pediatrics 2004;113(suppl 6):1907-1916.
- Bugeja L, Franklin RC. An analysis of stratagems to reduce drowning deaths of young children in private swimming pools and spas in Victoria, Australia. Int J Inj Contr Saf Promot. 2013;20(3):282-294. doi: 10.1080/17457300.2012.717086
- Dangerous waters: profiles of fatal childhood drowning in the US 2005-2014. Safe Kids Worldwide. June 2016. Accessed May 2, 2021.https://www.safekids.org/sites/default/files/dangerous_waters_research_report.pdf
- Quan, L., Ramos W, Harvey C, et al. Toward defining water competency: an American Red Cross definition. Int J Aquat Res Educ. 2015;9(1):12-23. doi:10.25035/ijare.09.01.03
- Stallman RK, Moran K, Quan L, Langendorfer S. From swimming skill to water competence: towards a more inclusive drowning prevention future. Int J Aquat Res Educ. 2017;10(2). doi:10.25035/ijare.10.02.03
- Graham RD. Comparative energy expenditure of drown proofing and treading water. Master’s thesis. University of Oregon; 1977.
- Fritzvold R. The comparative energy costs of treading water and survival floating. Undergraduate thesis. Norwegian School of Sport Science; 1986.
- Stallman RK, Junge M, Blixt T. The teaching of swimming based on a model derived from the causes of drowning. Int J Aquat Res Educ. 2008;2(4). doi:10.25035/ijare.02.04.11
- Bennett HJ, Wagner T, Fields A. Acute hyponatremia and seizures in an infant after a swimming lesson. Pediatrics. 1983;72(1):125-127.
Todd R. Porter, MD, MSPH, Nicole Hughes
Contemporary PEDS Journal, June 2021, Volume 38, Issue 6